Theoretically,
CEUS can be used to evaluate any tissue studied by conventional ultrasonography.
The characterization of FLLs is CEUS’ most established indication.
Unlike convencional ultrasonography,
CEUS characterizes patterns of enhancement on arterial,
portal and late phases analogous to those shown on contrast-enhanced CT and MRI,
allowing dynamic evaluation of FLLs vascular behaviour.
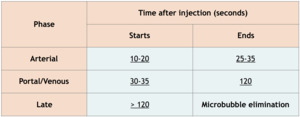
Table 1: CEUS contrastographic phases.
As microbubbles are purely intravascular,
there is no equilibrium phase.
This explains why there are some differences between late enhancement patterns of CEUS and contrast-enhanced CT or MRI.
On CEUS the only determinant for the intensity of enhancement is the vascular volume.
On contrast-enhanced CT or MRI,
however,
vessel permeability also has accountability.
Benign focal liver lesions
Benign FLLs are a common finding,
affecting about 20% of the population.
They are commonly detected by ultrasonography because of its wide availability.
CEUS can depict characteristic features that allow accurate characterization of these lesions,
thus reducing referrals to CT,
MRI or even biopsy if the lesion is described as benign.
However,
there are multiple benign FLLs and not all of them have characteristic features on CEUS.
Among the ones with characteristic vascular behaviour are hemangiomas,
focal nodular hyperplasia,
adenoma,
cysts and focal fatty deposit or sparing.
Hemangioma
Hemangiomas are the most common benign tumors of the liver,
with a prevalence of 0.4-7.4%,
female predilection and no malignant potential.
They can be isolated or multiple and are usually asymptomatic (except in rare cases,
when they are extremely large).
Histopathologically,
hemangiomas consist of capillary vascular bundles,
rich in fibrotic tissue / bands and with no capsule.
On conventional ultrasound,
they typically appear as well defined,
homogeneously hyperechoic rounded lesions that can sometimes exhibit posterior acoustic enhancement.
Large hemangiomas may have a heterogeneous structure due to ischemia and hemorrhage.
As the flow velocities inside them are very low,
they usually show no signal on Doppler mode.
In the presence of hepatic steatosis,
cirrhosis or patients undergoing chemotherapy,
the appearance of a hemangioma may alter and become “atypical”,
thus requiring further imaging for the diagnosis.
On CEUS,
their typical pattern is globular peripheral enhancement on arterial phase,
with progressive centripetal filling that usually completes during the late phase,
with a persistent isoechogenicity.
Large hemangiomas may have unenhanced areas that represent intralesional thrombosis or fibrosis.
Fig. 4: Small hemangioma on CEUS evaluation (arrows).
Fig. 5: Large hemangioma on CEUS evaluation (arrows). Note the unenhanced central area that corresponds to intralesional fibrosis or thrombosis.
Focal nodular hyperplasia (FNH)
Focal nodular hyperplasias are common benign liver tumors of the liver,
without malignant potential and frequently detected in women between 30 and 50 years old.
They are normally asymptomatic and can present as multiple lesions in 15-30% of the cases.
Histopathologically,
FNH is an area of normal liver cells proliferated around an arterialized scar,
characterized by the absence of the central terminal vein and by capillarization of the sinusoids.
On conventional ultrasound they appear as unspecific solid lesions without capsule.
Sometimes (especially in large lesions) the central scar can be identified as linear echoic structure.
In these cases,
the center vessel radiating from the center to the periphery can be seen on Doppler mode (highly specific finding).
On CEUS,
FNHs show hyperenhancement in the arterial phase,
with a typical fast centrifugal fill-in exhibiting a radial distribution (“spoked wheel” appearance).
On portal and late phases they become isoechoic.
Fig. 6: Focal nodular hyperplasia on CEUS evaluation (arrows).
Adenoma
Adenomas are rare benign hepatic tumors,
occurring mainly in young women using oral contraceptives.
Their clinical presentation is usually related to the mass effect of the lesion and pain due to intratumoral bleeding.
Malignant transformation may occur in 5% of the cases.
The risk of hemorrhage and the malignant potential are the main reasons why some adenomas are indicated for surgery.
Histopathologically,
an adenoma is an accumulation of large hepatocytes,
with poor connective tissue support and no biliary structures or Kupffer cells.
The vascularization is arterial without portal venous supply.
On conventional ultrasound,
they appear as a well-defined heterogeneous solid tumors that can be hypoechoic,
isoechoic or hyperechoic depending on the intratumoral fat and the underlying liver parenchyma.
The signal on Doppler mode is uncharacteristic.
On CEUS,
adenomas usually show moderate and heterogeneous hyperenhancement in the arterial phase,
with centripetal or diffuse filling (often described as “chaotic vessels”).
In the portal and late phases these lesions tend to become progressively isoechoic.
Sometimes,
however, they exhibit a mild washout that may cause misinterpretation of adenomas as malignant tumors.
Fig. 7: Adenoma on CEUS evaluation (arrows).
Focal fatty deposit and focal fatty sparing
Focal fatty deposits and focal fatty sparing are pseudo-tumoral areas usually located adjacent to the hepatic hilum,
close to the gallbladder or along the portal bifurcation.
The different fatty infiltration is due to the different perfusion characteristics of this areas.
On conventional ultrasound,
focal fatty deposits and focal fatty sparing are described as hyperechoic and hypoechoic areas (respectively) with geographic appearance and without mass effect.
There is no distortion of the vessels that run through this areas.
On CEUS,
these areas have the same enhancement as the surrounding liver parenchyma during all the vascular phases.
Fig. 8: Focal fatty sparing on CEUS evaluation (arrows).
Cysts
Hepatic cysts are common benign liver FLLs,
almost always asymptomatic and occurring in 2-7% of the population with a slight female predilection.
They can be isolated or multiple and have no malignant potential.
Histopathologically,
hepatic cysts are serous collections circumscribed by cuboidal epitelium.
On conventional ultrasound they appear as well defined anechoic lesions,
with a thin (often imperceptible) wall and posterior acoustic enhancement.
Few fine septa and some layering debris are relatively common,
but without wall thickening.
They show no signal on Doppler-mode.
Sometimes,
cysts may present abundant deposits and organization as a solid mass,
appearing as a hypoechoic tumor.
In these cases,
especially in patients with underlying cirrhosis,
it is important to exclude vascularity inside the lesion.
On CEUS they show no enhancement during any of the vascular phases.
Fig. 9: Hepatic cyst on CEUS evaluation (arrows).
Malignant focal liver lesions
One of the main applications of ultrasonography is the detection of malignant liver tumors,
particularly in patients with an increased clinical risk,
as it happens with underlying cirrhosis or when an oncologic context is known.
Neovascularity and arteriovenous communications are characteristic of neoplastic circulation and in CEUS these are expressed by the washout phenomenon.
Washout begins at the end of the arterial phase or during the venous phase,
it is persistent and has a specificity of 88% for malignant lesions.
Therefore,
the specificity of CEUS is high but not absolute,
with the final diagnosis being based on an accumulation of criteria,
which includes the clinical presentation,
biochemical data and the underlying liver characteristics (e.g.
cirrhotic or non-cirrhotic).
There are also a few studies that correlate the washout speed of a tumor with its aggressiveness,
attributing CEUS a prognostic value.
Among the malignant tumors with characteristic vascular behaviour are hepatocellular carcinoma (HCC),
metastases and intrahepatic cholangiocarcinoma (ICC).
Hepatocellular carcinoma (HCC)
Hepatocellular carcinoma is the sixth most common neoplasm and the most frequent primary tumor of the liver.
In the vast majority of cases (70-90%),
HCCs develop on an established background of chronic liver disease,
most of them with underlying liver cirrhosis.
They may present as a unique mass (focal),
as multiples masses (multifocal) or as an infiltrative pattern.
Histopathologically,
there is proliferation of neoplastic cells,
with a tumoral circulatory bed made of arterial vessels with disorganized distribution and arteriovenous shunts.
There is absence of Kupffer cells and loss of the normal connective tissue support.
On conventional ultrasound,
HCCs have variable appearance,
depending on their size,
degree of differentiation,
fat content and underlying liver echogenicity.
They can have a wide presentation spectrum,
from a small,
well-defined hypoechoic nodule,
to an ill-defined,
large heterogeneous mass with calcifications and necrosis or a diffuse infiltrative pattern which can be difficult to distinguish from background cirrhosis.
Sometimes a “basket pattern” can be identified on Doppler mode,
which represents the arterial vessels that circumscribe the tumor.
On CEUS,
HCCs show increased and diffuse enhancement in the arterial phase with washout during the portal or late phases.
The washout timing is related to the degree of cellular differentiation: well-differentiated HCCs tend to show late washout (which sometimes can be undetectable) while poorly differentiated HCCs tend to show rapid washout.
Fig. 10: Hepatocellular carcinoma on CEUS evaluation (arrows).
Metastases
Liver metastases are the most frequent malignant liver lesions,
arising mainly from gastrointestinal tract,
lungs,
breast and pancreas.
In the vast majority of cases they present as multiple lesions,
involving both liver lobes.
Hypovascular metastases are the most common (e.g.
from lung or gastrointestinal tract) while hypervascular metastases occur less frequently (e.g.
from melanoma,
renal cell carcinoma or neuroendocrine tumors).
On conventional ultrasound,
liver metastases have an extremely diverse appearance,
as they may develop haemorrhage,
areas of ischemia and necrosis,
fibrosis and/or calcifications.
They can present as hypoechoic,
isoechoic,
hyperechoic or cystic nodules,
sometimes exhibiting a “bull’s eye” or “target lesion” appearance (a peripheral halo probably related to a combination of compressed hepatic parenchyma and proliferation of neoplastic cells) which,
although common,
is relatively unspecific.
Doppler study usually does not bring any significant information.
On CEUS,
liver metastases show rapid washout,
with persistent hypoenhancement during portal and late phases.
During the arterial phase,
hypervascular metastases exhibit diffuse increased enhancement while hypovascular metasteses only enhance at the periphery of the lesion.
Fig. 11: Hypovascular metastasis on CEUS evaluation (arrows).
Fig. 12: Hypervascular metastasis on CEUS evaluation (arrows).
Intrahepatic Cholangiocarcinoma (ICC)
Intrahepatic Cholangiocarcinomas,
although relatively rare,
are the second most common primary liver neoplasms.
They arise from the small biliary ducts and usually occur in healthy livers,
with late clinical onset and nonspecific symptoms.
Patients with Caroli disease,
primary sclerosing cholangitis,
choledochal cysts and intrahepatic biliary lithiasis have increased risk for developing ICC.
ICCs are subdivided into three different types according to their morphologic characteristics: mass forming (the most common form),
periductal infiltrating and intraductal growing.
Histologically,
there is normally a marked fibrous stroma in the center of the lesion with abundant neoplastic cells at the periphery.
On conventional ultrasound,
early ICCs are usually undetectable,
with the diagnosis being made based on indirect signs,
such as dilated intrahepatic bile ducts.
Advanced ICCs typically present as an ill-defined hypoechoic mass without capsule,
adjacent to biliary structures.
The signal on Doppler-mode is generally weaker than the one detected in HCCs.
On CEUS,
ICC’s exhibit heterogeneous hyperenhancement in the arterial phase,
often described as irregular and peripheral (“rimlike”),
which relates to the pathologic features of the lesion described above.
During the portal phase there is washout with persistent hypoenhancement during the remaining portal and late phases.
Note that the characteristic delayed enhancement of ICCs fibrotic stroma on contrast-enhanced CT or MRI evaluation isn't depicted on CEUS.
This happens because of the different contrast pharmacokinetics,
as explained above.
Ultrasound contrast agents are purely intravascular,
thus not retained within the interstitial space.
Fig. 13: Intrahepatic cholangiocarcinoma on CEUS evaluation (arrows).

 for CEUS examination.")

.")
. Note the unenhanced central area that corresponds to intralesional fibrosis or thrombosis.")
.")
.")
.")
.")
.")
.")
.")
.")